Clot Recurrence Risk
The first priority when a venous blood clot happens is to start treatment promptly. Our goals are to decrease symptoms and to prevent complications. But then we need to make decisions about how long to anticoagulate for. Generally speaking, there are two options for treatment duration: short-term (usually 3 months) and extended therapy. And to determine treatment duration we typically consider patient symptoms, bleeding risk with extended therapy and clot recurrence risk.
Natural History of Venous Thrombosis
Without treatment clot recurrence over 5 years occurs somewhere between 1 and 50% of patients. Obviously, this is not a useful number. In order to advise patients, we need a better understanding of their recurrence risk. To do so, we need to consider various factors that affect recurrence risk. These factors are patient- and clot-related.
Factors Associated with Clot Recurrence
We know of several factors that are associated with clot recurrence. When assessing the need to continue anticoagulation, we need to take these into account. But, it is important to note that there are no standard tools to help us “accumulate” points for any specific patient. In other words, there are still common situations when we need to implement clinical judgement to decide about treatment duration.
Provoked, Unprovoked and Cancer Associated Clots
The most important factor by far is the circumstance that lead to the clot. When we can identify a transient modifiable risk-factor, such as trauma or surgery, the recurrence risk is the lowest. However, when we cannot identify such a cause, then recurrence rates are high. This is called an unprovoked clot. Finally, there is a strong connection between cancer and thrombosis. So, clots that happen in the setting of cancer posses the highest risk to recur if we stop treatment.
Male Sex
Males have a higher recurrence risk than females. In fact, some do not recommend long-term anticoagulation to non-obese women after a first blood clot, even if it was unprovoked. This is based on studies such as the HERDOO2 study.
Obesity
Obesity is an independent risk factor for clot recurrence. In fact, there is evidence that the connection has a molecular basis, rooted in pro-inflammatory and pro-thrombotic molecules.
Chronic Immobilization
Chronic immobilization is a tricky risk factor to assess. As you probably know, we do not offer prophylactic anticoagulation to chronically immobilized patients. For instance, wheelchair bound persons living in the community typically do not receive routine prophylactic anticoagulation. But immobilization is a more complicated state. First, not all immobilized patients are the same. For instance, spinal cord injury patients have especially high clotting risk. Second, immobilized patients reside in different locations. For instance, nursing care to move patients passively might be better at one place compared to another. Also, many immobilized patients have multiple medical conditions that promote both clotting and bleeding risk. So deciding how to address the excess clotting risk can be challenging.
Specific Medical Conditions and Clot Recurrence
Some patients will have medical conditions that can affect clot recurrence, and that do not fall into any of the other categories. Some of these conditions will be relatively transient, while others will be chronic. Assessing the exact status of the condition and tailoring treatment can be challenging, but important for appropriate care.
Pregnancy is one example. Anatomical and hormonal changes during pregnancy promote clotting. The post-partum period is also a risky time as far as clots. Once these periods pass, often the risk goes down, and we can consider stopping anticoagulation.
Another example are inflammatory conditions. A person might experience a clot during an exacerbation of an inflammatory disease. Treatment such as steroids can promote clots as well. Sometimes, the risk remains elevated for prolonged periods of time. But, if the disease is under control, the risk may become low enough to allow stopping anticoagulation. Deciding when that happens is not always simple.
Anatomical Defects
Often overlooked, anatomical considerations can be central to recurrence risk. First, varicose veins. We know that varicose veins are a risk for superficial clots and also for deep vein thrombosis. However, not all varicose veins are made the same. We probably need to take into account the extent of the varicose veins and whether there was actually a clot in them. If there was a clot, we should understand if it was in a peripheral, superficial varicosity, or if it was close to the deep system.
Next, is a popliteal vein aneurysm. In fact, there are case reports of patients who developed clot in these aneurysms and also of mortality for PE that came from these clots. Venous scarring is another, somewhat similar, cause. You will not find much literature about this. But some patients tend to have recurrences of clot in the same area and sometimes you can identify a history of trauma to that location.
Most infamous is iliac vein compression, also known as May-Thurner. An imaging finding of iliac vein compression is not rare. But we need to distinguish that from true compression with meaningful impediment to flow. It is not entirely clear if fixing a true compression is enough to reduce recurrence risk. But that is definitely the practice of some.
Finally, we need to mention IVC filters. Of course, these are not exactly an “anatomical” defect. But in some patients introducing a foreign body will increase the risk of recurrent clot. The mechanism is through obstructing blood flow and through mechanical effects on the blood itself that induce coagulation.
Deep Vein Thrombosis Location and Recurrence Risk
Distal deep vein thrombosis (calf vein thrombosis) will usually have a lower recurrence rate than proximal DVT. Also, pulmonary embolism will usually be on the higher side of recurrence. There is still some controversy about the implications of sub-segmental PE, however.
D-dimer and Clot Recurrence
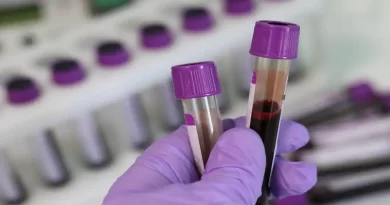
The most common blood test we use to assess recurrence risk is d-dimer. D-dimer is a breakdown product of fibrin. It is elevated in multiple conditions, but acute thrombosis is one of them. Specifically, elevated levels are also associated with recurrent thrombosis risk. While not specific, testing for d-dimer after stopping anticoagulation can help risk-stratify recurrence risk in patients who prefer to come off of anticoagulation. D-dimer is useful after unprovoked clots. While some clinicians use it after provoked clots, I don’t see the value there, because recurrence risk is low as it is.
Residual Clot
There is controversy in the literature about the role of residual clot in recurrence risk. A meta-analysis did not show that residual clot predicted clot recurrence risk. Another, patient-level meta-analysis, analyzed time-specific residual clot. Late residual clot (after 6 months or more) was not predictive of clot recurrence.
Known Thrombophilia
First, the bottom line: thrombophilia testing is usually not indicated. Now for some details. We know that some inherited or acquired changes in blood coagulation factors can increase the risk of an original thrombosis or recurrent thrombosis. But, in general, the magnitude of this effect is lower than that of other factors such as the clot circumstances or anatomical defects. Also, we realize that we do not know all the factors that are involved in recurrence. For instance, the prevalence of the Factor V Leiden mutation in the population is much higher than the risk of clotting in these patients. Another example is that there are families with recurrent clot where we cannot (yet) identify a specific cause. Taking all this together, for most patients, knowing other factors matters more than knowing about the thrombophilia.
Having said all that, in some select cases, considering a known thrombophilia can make sense.
Clot Location vs. Clot Recurrence
Clot location is not associated with clot recurrence, unless there is a specific anatomical defect. But, we still need to consider clot location when planning treatment. For many patients (and doctors) a pulmonary embolism is a worse outcome than most deep vein thrombosis. So if we knew that there was a higher likelihood for a PE compared to a DVT, that might affect our treatment algorithm. Indeed, it seems that generally, though not exclusively, clots tend to recur where they happened originally. You can read about it here (scroll down to “additional observations”). So if a patient had a PE, recurrence might be PE again. But still, remember that this is not exclusive.
Can we Assess Clot Recurrence in Specific Patients?
There are multiple tools out there to try to help us assess patient recurrence risk. Non of the tools are absolute. In other words, no tool will spit out if a patient will or will not have a recurrence. The best they can do is to offer an assessment of recurrence risk. Some tools focus on one factor (e.g., d-dimer), while other tools are more sophisticated, such as the post d-dimer tool or the HERDOO2 tool. Still, the 2020 American Society of Hematology guidelines specifically recommend against the use of prognostic tools, including d-dimer and residual clot (see recommendations 15, 16, and 17 here).